Why Cutting Psychologist Training Hours Risks Public Safety: Lessons from Medical Residency Data
- Dec 17, 2025
- 6 min read
Updated: Apr 27
Publication Date: December 17, 2025
Watch a 3-minute summary of this post on Youtube: https://youtu.be/9UChORtBIrQ
On Saturday, December 6, 2025, psychologists rallied in Ottawa and Toronto in protest of the College of Psychologists and Behaviour Analysts of Ontario (CPBAO)'s proposed cuts to training standards (CPBAO, 2025a). The proposed cuts would reduce supervised training hours by 75% (from approximately 6,000 to as few as 1,900), eliminate the oral exam, and remove the four-year work experience requirements for master's-level entry as psychologists. Additional changes to safeguards have already been implemented by the CPBAO - including replacing the traditional ethics exam with a low-stakes, no-fail online module (JEE), and expanding the number of attempts allowed on the Examination for Professional Practice in Psychology (EPPP) from a current limit of four per 12-month period to unlimited attempts (Psychology Advocacy Network, n.d.).
In a recent CTV News article (CTV News, 2025), CPBAO Registrar Dr. Tony DeBono positioned the proposal as modernization to address workforce shortages without compromising competency. Similarly, in the October 2025 HeadLines newsletter, the president of the CPBAO council, Dr. Ian Nicholson, framed concerns about "automatically registering incompetent providers" as a myth, asserting that the five core competencies - assessment, intervention, research, ethics, and relationships - remain unchanged (CPBAO, 2025b). He maintains candidates must still demonstrate independent practice readiness despite reduced supervised training hours, and implies that an equivalent level of competence is achievable.
In the analysis that follows, we examine data on medical resident complaints published by the Canadian Medical Protective Association (CMPA) as an evidence-based analogue for the CPBAO’s proposed cuts to supervised training in psychology. Both medicine and professional psychology balance risk, supervision, and autonomy under public trust. If the CPBAO’s proposal is adopted, Ontario psychologists will assume autonomy and responsibility much earlier in their training and credentialing. To understand the implications of reduced supervision, it is useful to examine professions that track competence and risk across training; medicine is particularly relevant because, like psychology, it entrusts early-career practitioners with vulnerable clients while gradually granting greater autonomy.
CMPA Overview: Why Medical Data Matters
To my knowledge, there are no longitudinal studies that track regulatory complaints about psychologists (or citations in court proceedings) across the various stages of supervised training or early independent practice in Canada. As a result, it is not currently possible to directly quantify risk levels among psychologists.
In contrast, the Canadian Medical Protective Association (CMPA), which assists member physicians with medico-legal issues that arise from their professional practice of medicine, maintains comprehensive, peer-reviewed data on regulatory complaints (CMPA, 2023). According to the Crosbie et al. (2022), over 95% of Canadian physicians identify as members.
Because both psychology and medicine depend on supervised training to develop independent clinical judgment, medical residency data offer a relevant evidence base for understanding early-career risk.
What CMPA Medical Complaint Data Show
A. Peak Complaint Rates Early in Training
Between 2008 and 2017, McDougall et al. (2022) found Ontario physicians-in-training were named in more civil legal cases than those in any other province (700 of 951 cases). When broken down by residency year, cases were highest in the earliest years (PGY1–PGY3) compared to later years.
A separate analysis of 142 closed regulatory complaints (2013–2017) showed complaint rates peaked in the first two years of residency but declined progressively with extended supervised experience (Figure 1; Crosbie et al., 2022).
In medical residency, physicians are licensed and responsible for patient care under the supervision of an attending physician. They perform advanced clinical tasks, make independent medical decisions, order tests and treatment, and supervise medical students and junior residents. They progressively gain more autonomy across each of the six years (PGY1 to PGY6). Residents complete medical school clerkships beforehand, but those involve limited responsibilities.
Figure 1: Number of Medical Residents Cited in CMPA Complaints involving Patient Care, 2013–2017 (Crosbie, et al., 2022, p. E38)

These findings reveal a clear pattern: the complaint rates peak during the earliest residency years (PGY1–PGY3), when supervision is most intensive and when autonomy is rapidly expanding. They also suggest that extended supervision plays a critical role in mitigating early-career risks before clinicians transition to independent work.
Applied to psychological practice, a policy that substantially reduces supervised training hours could elevate early-career risk, just as early medical residents show higher complaint rates.
B. Higher Harm Levels with Trainees
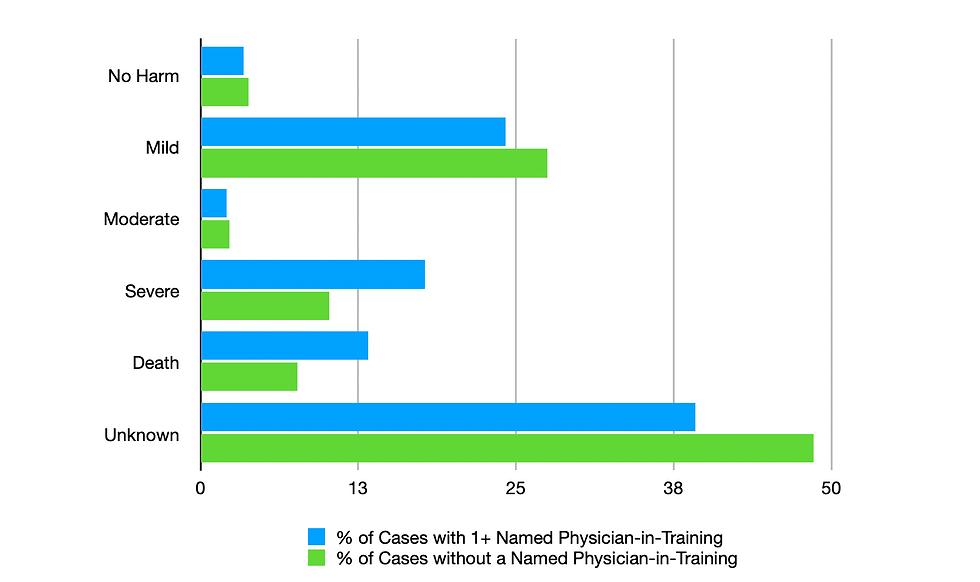
McDougall et al. (2022) found a greater proportion of civil cases involved severe harm or death when physicians-in-training were named compared to cases without trainees. While causality cannot be established, the authors recommended "tailored risk management training," particularly in high-harm specialties like surgery. The authors acknowledged that it is not possible to infer whether the patient harm was preventable, and their analyses were not designed to examine who provided substandard care. However, they suggested that greater attention to this type of training could help reduce risk, particularly where the potential for severe harm is highest.
Figure 2: Percent (%) of total cases by level of patient harm in medico-legal cases with (n=1107) and without (n=12703) a named physician-in-training among closed cases in the repository of the Canadian Medical Protective Association, 2008–2017 (McDougall et al., 2022, p. E785).
This principle applies directly to psychology: not all competencies develop at the same rate - some domains require more supervised repetitions. High-risk areas like suicide assessment, crisis intervention, forensic evaluations, complex personality disorders, and multiple comorbidities will necessitate targeted and extended supervision to protect vulnerable clients.
C. Assessment as Primary Risk Area
As shown in Table 1, the top two reasons for complaints were deficient assessment (49%) and diagnostic error (44%) (McDougall et al., 2022). Most cases (95%) resolved without severe sanctions, with 56% employing educational interventions. These data affirm the protective role of supervision in risk reduction.
Table 1: Top 10 reasons for complaints among Canadian Medical Protective Association college complaint cases involving residents and patient care, 2013–2017 (n = 142)
Reason for complaint | No. (%) |
1. Deficient assessment | 69 (48.6) |
2. Diagnostic error | 62 (43.7) |
3. Unprofessional manner | 41 (28.9) |
4. Communication breakdown, patient | 32 (22.5) |
5. Failure to perform test or intervention | 21 (14.8) |
6. Inadequate supervision | 16 (11.3) |
7. Inadequate consent process | 16 (11.3) |
8. Injury associated with health care delivery | 14 (9.9) |
9. Inadequate patient monitoring or follow-up | 13 (9.2) |
10. Sexual impropriety | 13 (9.2) |
Source: Crosbie et al. (2022), page E39.
Turning to psychological practice, the core competency of assessment mirrors medicine's highest-risk area. CMPA data show early-career assessment-related failures decline with extended periods of supervision. CPBAO's proposal to cut supervision hours by 75% while eliminating oral exams removes this essential "formative gradient" in competence development. At this time, no equivalent psychology dataset supports Dr. Nicholson's assumption of equivalent professional readiness.
Conclusion
In conclusion, although CPBAO leadership frames the changes to psychology licensing criteria as modernization, medicine's residency data suggest otherwise: reduced supervision elevates early-career risk in high-stakes domains. Without psychology-specific longitudinal evidence, Ontario risks undermining public safety and professional trust. Cutting Psychologist Training Hours Risks Public Safety is a warning that policymakers should take seriously.
References:
Canadian Medical Protective Association. (2023). Homepage. https://www.cmpa-acpm.ca/en/home
College of Psychologists and Behaviour Analysts of Ontario. (2025a, October 10). Consultation: Amendments to registration regulation 193/23 under the Psychology and Applied Behaviour Analysis Act, 2021 [Consultation document]. https://cpbao.ca/wp-content/uploads/Consultation-Amendments-to-Registration-Regulation-under-the-Psychology-and-Behaviour-Analysis-Act-2021-5.pdf
College of Psychologists and Behaviour Analysts of Ontario. (2025b, October). HeadLines: October 2025. https://cpbao.ca/headlines_issue/october-2025/
Crosbie, C., McDougall, A., Pangli, H., Abu-Laban, R. B., & Calder, L. A. (2022). College complaints against resident physicians in Canada: a retrospective analysis of Canadian Medical Protective Association data from 2013 to 2017. CMAJ open, 10(1), E35–E42. https://doi.org/10.9778/cmajo.20210026
CTV News. (2025, December 7). Psychologists rally on Parliament Hill against proposed cuts to training. https://www.ctvnews.ca/ottawa/article/psychologists-rally-on-parliament-hill-against-proposed-cuts-to-training/
McDougall, A., Zhang, C., Yang, Q., Taylor, T., Neilson, H. K., Nuth, J., Tsai, E., Lee, S., Lefebvre, G., & Calder, L. A. (2022). Patterns and trends among physicians-in-training named in civil legal cases: a retrospective analysis of Canadian Medical Protective Association data from 1993 to 2017. CMAJ open, 10(3), E781–E788. https://doi.org/10.9778/cmajo.20220075
Psychology Advocacy Network. (n.d.). Some changes are too risky to rush. https://www.psychadvocacy.ca/
Dedication: This blog is dedicated to the memory of a friend, writer, poet and entrepreneur, Mr. Anthony Iacovino. His kindness, humanitarianism, and thoughtfulness will be deeply missed.
Disclaimer: This article presents evidence-based policy analysis regarding public training standards. The views expressed are solely those of the author and do not constitute legal, professional, or medical advice. Readers should consult qualified professionals for personal guidance.


